
Personal Reflections on the humanitarian paradox in Syria
Throughout the humanitarian response in Syria, representatives from U.N. agencies, international and selected local organizations gathered every two weeks in Damascus’s luxury hotels and offices in the city’s richest neighborhoods to discuss the health and nutrition sectors’ programs. Coffee and tea were plentiful. Platters of pastries and fruit circulated through the room. No matter how many people had starved in the city’s besieged neighborhoods and rural towns a few miles away, the muffins remained fresh.
I often reflected on these paradox without fully understanding what disturbed me about it. At the time, I was working for Damascus-based humanitarian organizations, part of the internationally coordinated response operating from inside government-controlled Syria. I had returned to humanitarian work in 2016, several years after leaving the Syrian Red Crescent and completing my residency in internal medicine.
By then, the conflict had become part of the city’s sensory fabric. The daily shelling from Mount Qassioun folded into the ordinary noise of Damascus.[i] Airstrikes hit Eastern Ghouta, Yarmouk Camp, and the rural towns surrounding the capital, including my mother’s hometown, where she is buried. These explosions existed alongside the established routines of life under an authoritarian state: long slow queues at checkpoints, crowds competing for subsidized bread, passengers kneeling inside overcrowded minibuses, and the constant humiliations of petty corruption in every bureaucratic interaction. In Damascus at that time, every stage of life required informal payments coupled with the suppression of humiliation and anger, from issuing birth and death certificates to obtaining passports. Each transaction demanded not only money but also emotional performance, manifested as animateness, to curb the self from moving toward repulsion and facing deadly state repression.
I joined the Red Crescent in 2007 as a medical student because I was searching for a sense of belonging and value. Few institutions in Syria allowed meaningful interactions across class, sect, and geography the way the Red Crescent did then. Through it, I encountered a broader Syrian society than that available through the university, mosque, school, or other social institutions accessible to ordinary citizens. The Red Crescent reconfigured my relationship with society around mutual respect and shared labor toward the public good.
That experience became decisive during the early months of the 2011 uprising.
Alongside other first aid volunteers, I found myself standing behind protest lines, carrying first-aid kits into demonstrations that could be attacked within minutes. Sometimes we evacuated wounded protesters before the security services sealed off an area, aided by the legitimacy of the humanitarian emblem, as well as by chaos and weak coordination among security, the police, and anti-riot troops. Many times, the ambulance cars provided first aid to the police and security agents too, mostly coming with heat exhaustion and minor wounds from falling. As the state’s grip grew firmer, however, the security apparatus ensured that ambulances and first aid providers could not intervene without prior approval. Still, many of us defied those restrictions, relying on informal networks to continue providing first aid and, eventually, surgical support in neighborhoods the government had decided to collectively punish.
Being on the streets gave me a clear understanding of the source of the harm and what needed to be done. These convictions sustained me through my arrest and forced disappearance in early 2012. I believed, with clarity, that I had done nothing wrong. My sense of certainty was grounded in the purpose that had initially drawn me to the Red Crescent and in the moral coherence of responding to visible suffering and witnessing the palpable impact of my skills and actions.
What shattered that clarity was not the detention center and its torture. It was the humanitarian apparatus itself, with its distant mode of sense-making and engagement on the ground.
By 2016, the internationally funded response in Damascus had reached its peak in both scale and budget. Yet my days felt detached from the catastrophe unfolding around us. I spent most of my time filling Excel sheets and reports’ templates, attending countless coordination meetings. Outside the office and public institutions, I occasionally visited primary care rehabilitation project sites, conducted health facility assessments, and, when permitted, spoke with facility workers. The work was less emotionally engaging than my years with the Red Crescent or in the emergency departments of public hospitals, even as the conflict itself had become far louder and more destructive.
Much of Damascus continued operating according to routines of survival. People worked, commuted, haggled over fuel and food prices, and queued for bread. Humanitarian workers performed another routine in parallel: conducting assessments, organizing capacity-building workshops, calculating indicators, drafting procurement plans, writing donor reports and proposals, and convening coordination meetings. These activities took place in secure, temperature-controlled, and furnished offices and cars insulated from the reality outside. Participating in the institutional culture involved wearing the agency’s logo, carrying an extra mobile, laptop, and notebook. These substituted my first aid kit and the Red Crescent uniform. The two worlds rarely interacted without the state’s oversight, yet one was supposed to understand and intervene on behalf of the other in its suffering.
Despite the intensification of the siege and news of starved women and children on social and international media, there was little hope that an international response can intervene against the regime will. International humanitarian actors were kept away from affected population through complex bureaucratic procedures and security measures, that culminated when successful with a letter guaranteeing their safety on checkpoints. These restrictions limited the flow of aid toward people and information flow toward aid agencies. Nonetheless, the Damascus-based response needed to preserve the appearance of functionality and impact. Maintaining that appearance required filtering out large parts of reality from the official gaze. Starvation in areas surrounding Damascus was subject to a slow verification process that could only be conducted once the Ministry of Foreign Affairs, the Ministry of Health, the Red Crescent, and the security apparatus had all been informed and approved the convoy’s plan, aid contents, and personnel list. These restrictions were justified by the regime’s denial of the siege and starvation, which it framed as politically motivated fabrications or isolated incidents by external actors to delegitimize the state.
The convoy approval process took months, and permission was granted at least in the areas facing the most severe deprivation. Even when convoys were authorized, their contents remained subject to extensive revisions and deletions, with medical and nutritional supplies routinely removed from distribution lists before departure. In many ways, this bureaucratic process of delay, negotiation, and removal became part of how siege itself operated.
When reports emerged documenting the removal of medical supplies from aid convoys to besieged towns, the agencies involved stopped publicly releasing detailed inventories. Instead, medical supplies began to be reported by aggregate weight. Pediatric antibiotic suspension bottles and high-energy biscuits were grouped together with wheelchairs and other heavy non-life-saving equipment, obscuring the actual composition and therapeutic value of the aid being delivered. There are no reports or data on the total calorie content of food parcels or other nutrition supplies throughout the response in Syria. There is no information on how much aid was imported into the country, where it was delivered, and what happened in the last mile before households received it.
Instead, indicators based on estimates rather than actual measurements were used to assess aid impact. For example, the percentage of the population reached in each town was calculated using an estimated population, based on the understanding that each delivered food parcel is meant to feed around 5 people for a month. No actual documentation of who received or did not receive aid took place. Furthermore, nutrition surveys in government-controlled areas excluded most of the areas the state besieged or had regained.
During coordination meetings, I could sometimes hear shelling from outside the hotel windows. Airstrikes were visible from certain offices. Yet humanitarian life often seemed insulated from the meaning of those sounds. I remember a discussion around sexual violence where an organization presented the achievement of its survivors-support program.
As the program metrics were being presented, I thought about a young woman who was admitted to the public hospital where I worked with a story of fever and altered mental status. She had just left Al-Hajar al-Aswad, a neighborhood in the south of Al Yarmouk camp that was besieged, with her sister. The nurse refused to insert a urinary catheter given that the girl was unmarried. When the urinary resident eventually performed the procedure, he quietly informed me about pelvic injuries the woman had. I did not ask her sister what happened. The fear on her face conveyed all that I needed to know. The patient died of septic shock several days later. I could not document the injuries nor report what I believe had occurred, knowing the dire consequences for both the patient’s sister and me. Cases like this escaped the attention of the health and humanitarian systems.
After the siege on Eastern Ghouta was tightened in late 2013, repeated warnings about worsening hunger and water insecurity produced little humanitarian response. International attention shifted only in late 2014, after images and videos circulated of a young girl with screw worm-infested head wounds. Advocacy groups in the diaspora used the footage to draw attention to the collapse of water and sanitation systems affecting nearly 400,000 people in the besieged enclave. The case prompted a public statement from the Damascus-based international response, which negotiated a convoy into Eastern Ghouta.[ii] In November 2013, cases of polio were confirmed in the eastern provinces, Aleppo, and one case in Eastern Ghouta led to mounting international pressure to carry out a national vaccination campaign across the conflict lines. Vaccination campaigns were coordinated and implemented largely in isolation from other health and nutrition operations.
I remember another patient, an elderly person admitted to the emergency department with an altered mental state and life-threatening uncontrolled diabetes. He had been sleeping in a public park for days after fleeing southern Damascus. He had an extremely foul smell, and upon examination, he had a screw worm infestation between his thighs. The nurses secretly reported him to the police. It later emerged he was wanted for a series of robberies in his coastal hometown, and he had been hiding in southern Damascus from before the conflict. Stories like his, shaped by displacement, poverty, illness, criminalization, and social collapse, rarely fit the dominant humanitarian narrative of state versus non-state violence. As a result, they disappeared from both public discourse and institutional response.
The humanitarian system struggled to recognize suffering that existed outside these simplified classifications of conflict exposure. Hundreds of displaced families had moved into informal settlements within Damascus itself after fleeing besieged suburbs and rural towns. At night, I watched women move between grocery stores looking to buy discarded vegetables cheap enough to cook. Others searched through trash containers. Hunger was not confined behind front lines. Yet the architecture of humanitarian response rendered many forms of deprivation invisible unless they aligned with the political logic governing access to aid.
| Table 1: list of major occurrences of starvation throughout the Syrian conflict 2012-2024 | ||||
| Location | Siege start -end | Approx. duration | Est. population under siege | Documented starvation deaths (by who) |
| Al-Yarmouk Palestinian camp | Jul 2013 – partial access 2014; enclave remained restricted until 2018 | 2013–2015 acute; restrictions to 2018 | 18,000 trapped in early 2014 (Palestinian refugees and Syrian) | 128 deaths (Amnesty International) in 2014. |
| Madaya | Jul 2015 -> Apr 2017 (Four Towns evacuation) | 21 months | 33,800–43,000 (locals + IDPs) | 65 starvation/malnutrition deaths (MSF) 2016 |
| Darayya | 2012 _ Aug 2016 (forced evacuation) | 4 years | 2,500–4,000 remaining by Aug 2016 (from a much larger pre-war city) | No reliable consolidated figure |
| Moadamiya al-Sham | 2012–2013 tightening -> 2016 surrender/evacuations | 3–4 years | (45,000; fell to a few thousand by surrender) | Several reported; at least 16 deaths from lack of food/medicine reported in 2013 (news/NGO reporting) |
| Esten Ghouta towns | 2013 tightening -> Apr 2018 capture | 5 years | 390,000–420,000 | No consolidated, authoritative count (widespread acute malnutrition documented) |
| Old City of Homs | 2012 -> May 2014 truce/evacuation | 2 years | (tens of thousands earlier; dwindled by 2014) | Deaths from starvation reported; no firm published total |
| Eastern Aleppo | Encirclement late Jul 2016 -> Dec 2016 fall | 5 months | 250,000–300,000 | No consolidated starvation count (severe shortages & last rations documented) |
| Foah & Kafraya | Mar 2015-> Jul 2018 evacuation | 3+ years | 16,500 | No consolidated starvation count |
| Zabadani | Jul 2015 -> Apr 2017 (Four Towns deal) | 21 months (after earlier fighting) | 700 (population shrank heavily; many displaced) | No consolidated starvation count |
| Deir Ezzor | 2014–2015 ISIS encirclement -> Sept 2017 relief | 2–3 years | 90,000–100,000 reliant on WFP airdrops (varied) | No consolidated starvation count (airdrops mitigated worst famine risk) |
Despite the enormous funding directed toward food assistance operations, there was little information about how much aid was distributed, to whom, and with what nutritional impact. No one denied that food insecurity continued worsening as social support systems collapsed, even in areas where active fighting had subsided.
My mother’s family lived only ten minutes outside Damascus. Before the conflict, generosity and mutual aid shaped everyday life there. During the summer pumpkin season, farmers gifted pumpkins away instead of selling them. Neighbors with cows sent my grandmother fresh colostrum after calves were born. In return, a child used to knock on our door to borrow onions, parsley, or bread missing from that day’s meal.
After my release from detention in late 2012, my visits became infrequent. When the siege cut us apart in 2013, we communicated mostly through WhatsApp. But as conditions worsened, conversation itself began to feel meaningless. The distance between us could no longer be bridged through ordinary language.
Men rarely admitted fear. They certainly did not talk about hunger.
Still, I knew what was happening. At least, my cousins were among the fortunate ones because they could still cultivate a small family plot of land. I heard stories of bread baked from animal feed, underground mushroom farms growing, raising rabbits instead of chickens, and, on the worst days, cooking grass and tree leaves. In the few photographs they shared, I watched their hair turn gray and their faces thin into unfamiliar versions of themselves.
Carrying that knowledge became exhausting.
Beneath the fear of re-arrest and the pressure to appear competent and composed in professional humanitarian spaces, often dominated by expatriates and members of Syria’s growing humanitarian class, there was another burden: the knowledge that I could do almost nothing for the people I loved. Around us, humanitarian work increasingly became a source of stability and wealth for a small professional elite earning fixed salaries and per diems unimaginable to most Syrians, but from the inside it felt like a straitjacket.
Over time, hunger itself slipped from my daily thoughts, overwhelmed by concerns about survival, work, and maintaining a place in a society losing its social fabric. I remained in indirect contact with my cousins after I left the country through relatives living abroad, until the siege was lifted after a horrific military campaign in 2018. Not all of them survived the conflict.
Knowing and remembering the details of their suffering has become unbearable. Especially when we are far. We prefer to talk about our children and complaints of daily life these days.
Yet my personal experience paralleled a broader institutional condition across the humanitarian sector in Syria. There remains remarkably little systematic public data on nutrition and health outcomes. No unified national health facility list exists. Population-level studies are scarce, and only one indirect mortality survey has been conducted throughout the conflict.[iii] At the same time, enormous resources flowed into advocacy campaigns and the documentation of individual violations. The humanitarian system became highly skilled at describing suffering to external audiences while remaining far less capable of measuring, understanding, or ensuring effective response and sustainable health outcomes.
Figure‑1 Map of starvation locations in Damascus and its countryside.
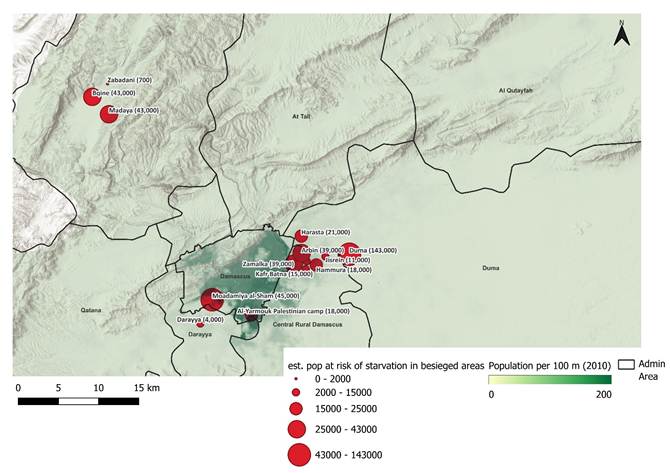
Population estimations are from Whole of Syria nutrition March 2016 update. Available at https://reliefweb.int/map/syrian-arab-republic/syria-wos-nutrition-reach-htr-bsg-areas-jan-mar-2016
[i] https://www.theguardian.com/world/2015/sep/13/danger-death-never-far-away-damascus-syria
[ii] https://www.reuters.com/article/world/tropical-fly-borne-illness-reported-near-damascus-who-idUSKCN0JB0XX/
[iii] Alrashid Alhiraki O, Fahham O, Dubies HA, Abou Hatab J, Ba’Ath ME. Conflict-related excess mortality and disability in Northwest Syria. BMJ Glob Health. 2022 May;7(5):e008624. doi: 10.1136/bmjgh-2022-008624. PMID: 35589154


